If you’re a marketing leader or executive at a DSO, you’ve probably noticed that, at some point, your paid media efforts seem to hit a ceiling and you can’t tell if your campaigns are actually leading to production.
(At least, the marketing leaders I talk to notice this in their DSO patient acquisition setup.)
This ceiling has nothing to do with budget, creative, or campaign structure. It exists because most DSO paid media systems are optimizing for the wrong thing: the lead. When really, you should be optimizing for appointments.
Why? Because your business goal isn't a lead. It's a patient who shows up, receives care, and generates production. That gap, between the signal you're measuring and the outcome you actually want, is where hundreds of thousands in marketing spend go to waste. It's the same core problem behind why so many DSOs can't connect ad spend to contracted patients.
This article explains what's actually happening, what needs to change structurally, and how to know whether your current setup has this problem.
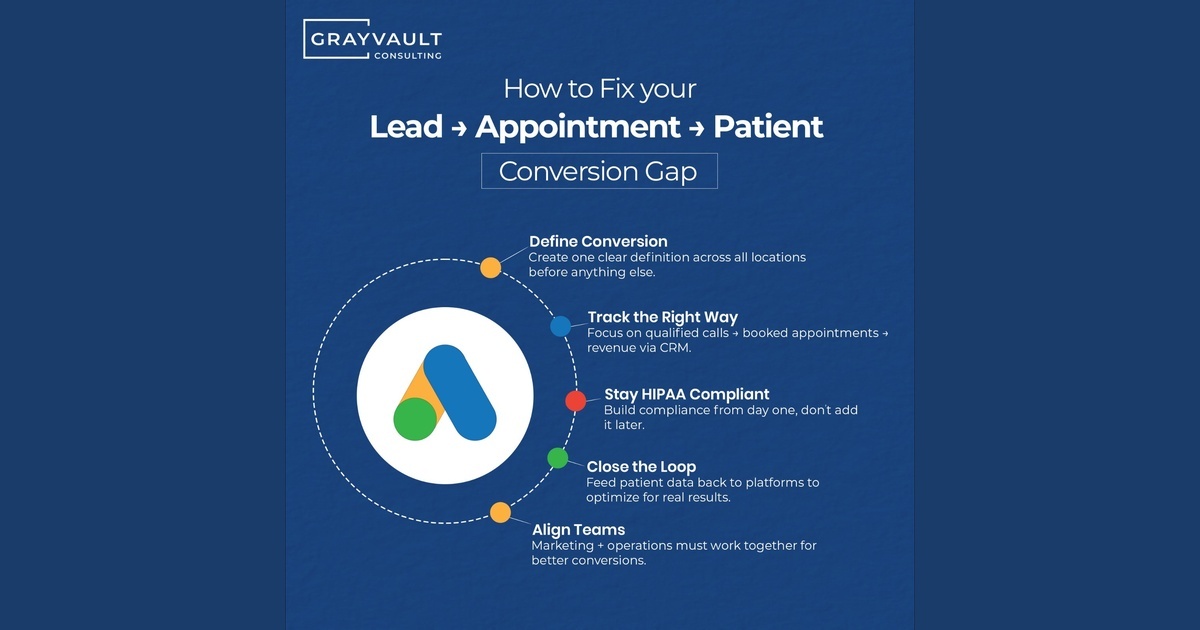
Why You Can't Scale Your Paid Media: You Have No Shared Definition of a Conversion
The first thing I encounter when working with a new DSO is that no two locations define a conversion the same way.
At one practice, a conversion might be any inbound phone call. At another, it’s a phone call longer than 30 seconds. At a third location, it’s a contact form submission. Across a group of 50 or 100 locations, you can have dozens of different definitions operating simultaneously inside the same ad platform, all feeding the algorithm conflicting data about what success looks like.
The downstream effects are significant. Nobody can determine if anyone is achieving success at the upstream level because nobody’s measuring the same thing to begin with. All of that leads to performance chaos and tons of wasted spend.
To solve this, start with a single, clear definition of what a quality lead looks like across your entire organization. A reasonable baseline might be a phone call of at least two minutes or a new patient booking. Everything else — contact form fills, calls under a certain threshold — should be treated as secondary signals at best.
The Six-Stage Patient Acquisition Funnel (Most DSOs Only Track at Stage One)
Once you have a unified definition of what a good conversion is, the next question is: what comes after the lead? This is where most DSO marketing systems fall flat.
The full patient acquisition funnel looks like this:
- Lead — a form fill, phone call, or ad conversion
- Call — was it answered? How quickly? By whom?
- Appointment — was it scheduled, and how far out?
- Show — did the patient actually arrive?
- Treatment — was case acceptance completed?
- Production — were services billed for?
DSO marketing teams tend to optimize exclusively for step one. Some reach step two. Few track steps three, four, or five. And virtually none are feeding that downstream data back into their ad platforms.
The goal of every person involved in marketing, especially paid media, isn’t to just make the phone ring. It’s to generate production and make sure that the right patient connects with the right clinic, gets the care they need, and creates production. When that becomes the shared goal across your entire marketing organization, you build systems that are structured to achieve it. If the phone rings but the booking never happens, the breakdown is often in where your intake process quietly loses patients.
The Conversion Tracking Infrastructure Behind Appointment-Level Optimization
Getting downstream conversion signals back into Google Ads requires two foundational layers: compliance infrastructure and CRM connectivity.
Layer 1: A HIPAA-Compliant Customer Data Platform (CDP)
Any growing or mid-to-large DSO needs a HIPAA-compliant CDP in place before attempting to pass patient-adjacent data back to ad platforms. Google Ads has never signed a Business Associate Agreement (BAA), which means patient data can’t flow directly from your CRM into Google without going through a compliant intermediary.
A HIPAA-compliant CDP solves this by acting as the intermediary layer. The CDP signs a BAA with you directly, taking on responsibility for the governance and security of data passing through its systems. With that layer in place, all of your marketing pipelines, paid media data, and CRM signals can flow through one centralized, clean, compliant platform before being passed back to Google or Meta. For a full breakdown, see the HIPAA-compliant stack you need.
The practical benefit extends beyond compliance. Having all your disparate marketing systems consolidated through a single platform makes workflows simpler, reporting more consistent, and optimization more effective. It removes the excuse for inconsistency.
Layer 2: CRM Connectivity and Offline Conversion Uploads
Once your CDP is in place, the next requirement is a CRM that can pass downstream signals back into your ad platforms. For enterprise-scale DSOs, Salesforce is one of the strongest options as it offers the degree of customization and technical architecture that a complex multi-location operation typically needs.
The mechanism is either offline conversion tracking for dental practices or, ideally, a direct API connection. With an API connection, data flows continuously from your CRM back into Google Ads — appointment shows, contract signings, production amounts — giving the system a live, ongoing picture of what your marketing is actually generating. This is the same architecture we walk through in how we connect ad clicks to contracted patients and production.
When you can pass production directly back to Google Ads, you unlock an entirely different tier of bidding capability. The algorithm now has the feedback loop it needs to optimize toward the outcomes your organization is actually trying to achieve. That is enterprise-grade conversion tracking.
Setting Up Appointment Tracking as a Primary Conversion Action
With the infrastructure in place, the conversion action hierarchy inside Google Ads should follow a clear progression. The goal isn't just to optimize for appointments, but to work toward closing the loop all the way back to production (substituting for revenue).
Start with phone calls, but set a minimum time threshold. Two minutes is a reasonable baseline for indicating a meaningful conversation actually happened. This alone will significantly improve signal quality compared to tracking all inbound calls.
Prioritize online appointment booking as your primary conversion action. If your website doesn’t have a booking From there, prioritize online appointment booking over lead form submissions. An online booking produces a far more relevant signal to both the user and the ad platform than a contact form fill ever can. Once booking is in place, demote lead form submissions to secondary status, or eliminate them as a tracked conversion altogether.
But appointment bookings are a waypoint, not the destination. The practices that get the most out of their paid media are the ones feeding downstream data back into the platform — did the patient show up? Did they sign a contract? Did that contract generate production?
When you can pass revenue data back into Google Ads through dental appointment tracking or a CRM API connection, the system gains the feedback it needs to optimize toward your actual business goals. This is what separates a functional paid media setup from one that compounds over time. It also depends on setting CPA and ROAS targets against real patient value.
What You Can See — and Do — With Better Data
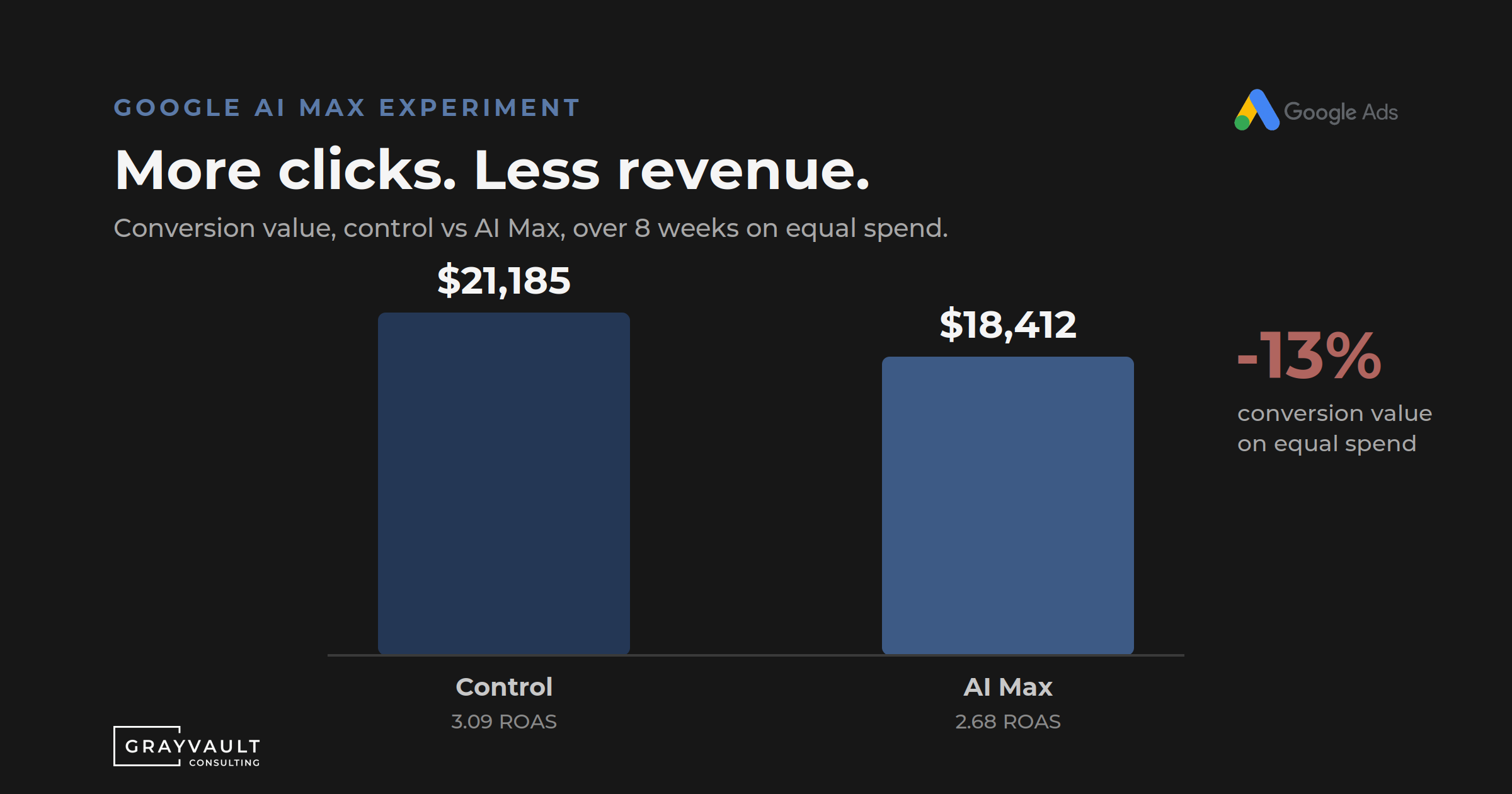
The difference between a lead-optimized account and an appointment-optimized account is far from subtle.
With lead optimization, you know which campaigns generated form fills and calls. But you don’t know which of those calls produced actual patients, which keywords are driving production, or whether your media spend is generating any real business outcome.
With appointment and production optimization, you can see exactly which campaigns had a role in generating downstream, business-level outcomes. You can trace your DSO paid media attribution all the way to the keyword and search term level.In aggregate, over time, patterns emerge that show you precisely what targeting is driving the results you want, not just the clicks.
More importantly, you’re also training the platform. When you give Google Ads signals that show down-funnel outcomes, the algorithm begins recognizing patterns across hundreds of variables — location signals, timing, device types, keyword combinations, audience characteristics — that no marketing analyst could parse manually. The system starts automatically bidding more heavily on the combinations most likely to drive production. That’s the compounding advantage that comes from getting the data layer right.
For leadership, the ROI case becomes hard to dispute. When you can tie media spend directly to production outcomes, you’re not presenting a marketing performance report. What you’re presenting is an attribution model that shows return on investment at the campaign level. And that changes the conversation entirely. This is exactly the kind of system we help build for multi-location healthcare organizations.
How to Audit Your DSO's Patient Acquisition and Conversion Tracking Setup
If you work with an in-house team or an external agency and want to know whether this problem applies to your accounts, conduct a paid media audit and start by looking at your active conversion actions. Work through this checklist:
- Are we tracking phone calls? If yes, is a minimum call duration threshold set?
- Are we tracking lead form submissions? Is there an online booking system that could replace them?
- Is appointment booking set as a primary conversion action, or is it absent entirely?
- Are we tracking appointment show rates? Is that data connected back into Google Ads?
- Are we tracking contract signings or treatment plan acceptance?
- Is production or revenue being passed back to the platform?
- Do all locations and practices share a single, consistent definition of what counts as a conversion?
If the answer to most of those questions is no, you’re measuring the top of your funnel and assuming the rest will take care of itself. In my experience, it won’t.
The good news is that you can solve this. The infrastructure exists, the platforms support it, and the methodology is clear. The harder work is internal: getting alignment across teams and locations on what the real goal is, and building systems structured around that goal from the ground up.
The Bottom Line
Paid media rarely stops working when you reach a certain budget. It stops working when the signal you are optimizing for stops representing the outcome you actually want.
Before you change your media mix, increase your budget, or hire a new agency, audit your conversion funnel at every stage. Find out where the signal ends. Build the infrastructure to extend it further. Then give your ad platform the data it needs to actually do its job.
Not Sure Where Your Signal’s Breaking Down?
The most useful thing you can do right now is work through the audit checklist above and find the first question you can’t answer confidently. That’s almost always where the real problem is sitting.
If you want a second set of eyes on it, that’s exactly the kind of conversation we’re set up to have — not a sales call, just a focused look at where the system breaks down and what it would take to fix it. Schedule a free consultation with me here.
Frequently Asked Questions
- What is the difference between optimizing for leads vs. appointments in dental paid media? Lead optimization tells your ad platform to find people who fill out forms or call. Appointment optimization feeds downstream signals — actual bookings, show rates, production — back into the platform so it learns what a valuable patient looks like, not just a click.
- Do DSOs need a HIPAA-compliant CDP to run Google Ads? Any DSO passing patient-adjacent data between systems needs a HIPAA-compliant CDP in place first. Google Ads does not sign a BAA, so patient data cannot flow directly from your CRM into Google without a compliant intermediary layer.
- How do you track appointment show rates in Google Ads? Through offline conversion uploads or a direct CRM API connection. When a patient shows up for their appointment, that event is passed back to Google Ads, allowing the algorithm to optimize toward the audiences most likely to actually arrive.
- Why is cost-per-lead a misleading metric for DSOs? Cost-per-lead measures the top of the funnel only. It tells you nothing about whether those leads became booked appointments, showed up, accepted treatment, or generated production. A low CPL can coexist with extremely poor return on ad spend.
- What CRM is best for multi-location DSO paid media attribution? For enterprise-scale DSOs, Salesforce is one of the strongest options due to its customization capability and technical architecture. The key requirement is that the CRM can pass downstream conversion signals back into Google Ads via offline uploads or API.
.svg)



.svg)
.png)

.svg)