A systems-first guide to Google Ads for multi-location healthcare organizations and DSOs. Learn how attribution, compliance, and conversion architecture determine scalable growth.
Craig Graham
•
July 4, 2026
A Systems Framework for DSOs
If you have ever attempted to scale Google Ads or other paid media platforms (vertically, horizontally, or both) across a multi-location healthcare organization, you likely faced many challenges. Some of these challenges could include budget allocation questions, attribution gaps, operational constraints, data processing errors, targeting overlap, and others.
However, all of these examples are components of something larger. Budgeting, attribution, execution of in-platform optimization, conversion tracking configuration and maintenence, etc are all components of a system.
In our experience, scaling Google Ads across multiple healthcare locations is rarely the result of one component, and is instead more likely a holistic systems problem.
For DSOs and multi-location healthcare organizations in the United States, Google Ads can absolutely drive growth. But as complexity increases (i.e. multiple providers, markets, compliance layers, CRM integrations) performance becomes dependent on system structure.
If a 40-location DSO engaged us tomorrow, we would not begin by tinkering with campaign settings.
We would begin by evaluating the integrity of the system.
Across DSOs and healthcare brands, underperformance usually stems from structural gaps rather than tactical mistakes.
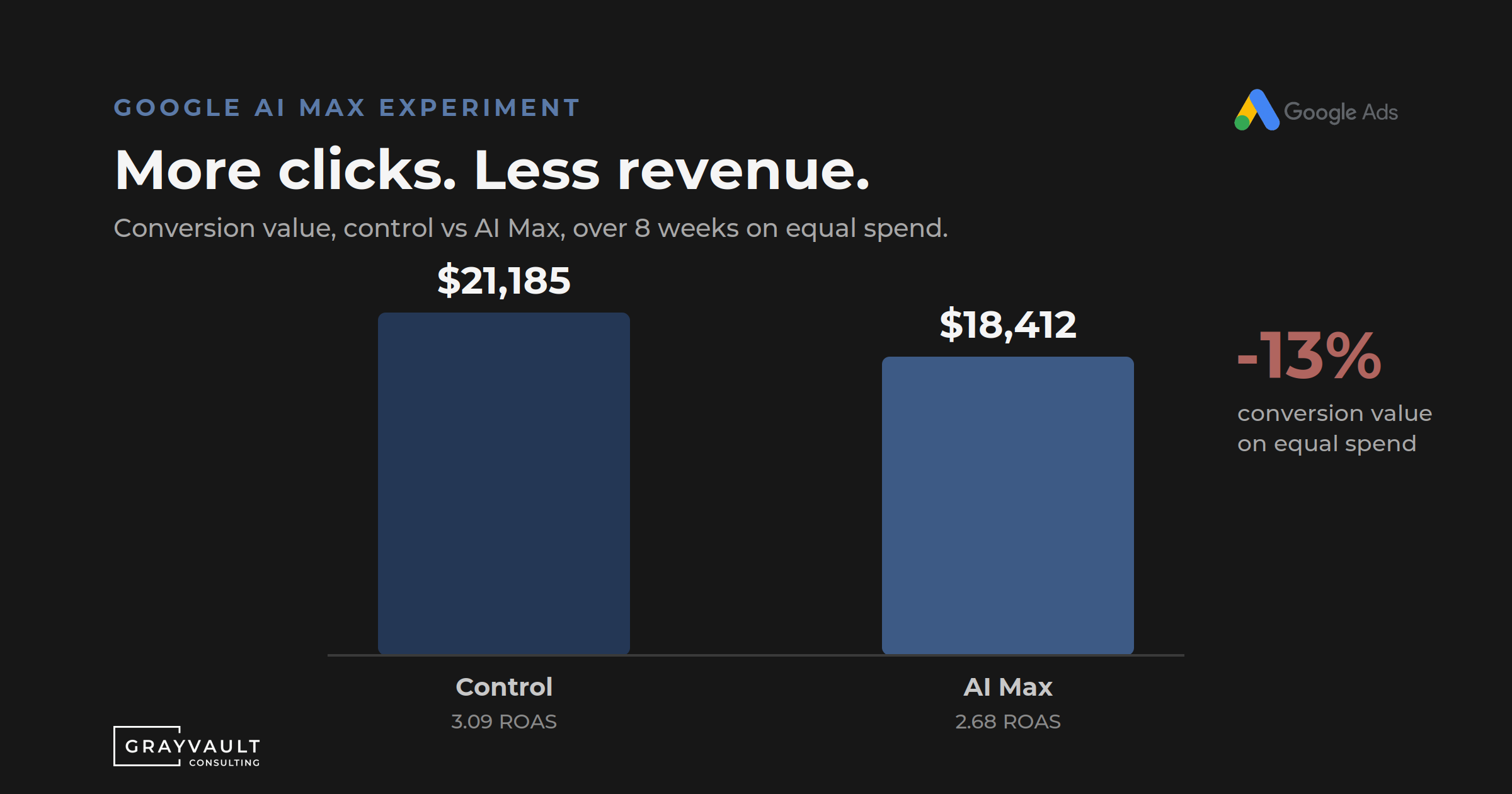
1. Platform Conversions Are Treated as Business Outcomes
Google Ads optimizes around the conversion actions you define.
If those conversion actions do not meaningfully ladder toward real business outcomes (scheduled appointments, attended visits, production revenue) the platform optimizes toward proxy signals.
That can appear to work at small scale, possibly only directionally (depending on the complexity of the setup).
But it breaks at enterprise scale.
In orthodontic and many DSO environments, those downstream milestones are often referred to as:
Case start (appointment scheduled)
Case start dismissed (appointment attended)
Contract start (treatment initiated and revenue generated)
In broader healthcare, terminology varies. The principle does not.
Enterprise-grade paid media requires outcome feedback loops. That often includes CRM integration, offline conversion uploads, and HIPAA-compliant infrastructure.
Without that, scaling becomes speculative.
2. Budget Is Treated as an Immediate Lever
Increasing spend does not instantly increase patients.
Algorithmic systems require stability. Large budget shifts can destabilize learning models, distort patterns, and introduce volatility.
Those lags must be incorporated into financial modeling.
Scaling responsibly requires pacing, planning, and executive patience. It is worth noting that executives often feel pressure to increase spend when performance plateaus. But without structural clarity, pressure creates volatility and can hinder growth.
3. Uniform Expectations Across Non-Uniform Markets
Not every location performs equally.
Brand equity, provider reputation, competitive density, demographic differences, and historical marketing presence all influence performance.
A systems-first approach respects that variance. It does not force uniform efficiency expectations across structurally different markets.
4. Structural Drift and Location Targeting Complexity
Location targeting is imperfect.
Overlap between markets, shared budgets, blended conversion learning, and inconsistent structure can distort data signals.
Account architecture must reflect business architecture.
Whether that means:
One account per location
A consolidated account with segmented campaigns
Portfolio bidding strategies
Or hybrid models
… depends on the brand’s operating structure, not platform convenience.
5. Expecting Attribution to Be Perfect
Healthcare attribution is rarely (if ever) perfect.
But it can be materially improved.
With disciplined conversion hierarchies, structured call tracking, CRM integrations, and offline conversion uploads, multi-location healthcare brands can move significantly closer to production-level visibility.
Attribution gaps are usually design failures, not platform failures.
What We Evaluate in the First 72 Hours
If we inherited 50 Google Ads accounts, the first three days would focus on clarity, not optimization.
Day 1: Governance and Risk
Who owns the accounts?
Does the organization have administrative control?
Are scripts or automated rules manipulating budgets?
Are conversion definitions coherent and layered?
Is there HIPAA-compliant data flow between systems?
A lack of transparency is a structural risk.
Advertising data should belong to the organization. Period. Full stop. It is a massive risk to engage with agencies that claim ownership over the data someone else paid for.
Day 2: Structural Integrity
Consistent naming conventions
Logical separation of brand and non-brand
Intentional match type usage
Organized negative keyword architecture
Strategic use of Performance Max
Properly configured location extensions
Call asset scheduling aligned to operating hours
Organization is a discipline signal. And discipline creates stability.
Day 3: Performance Alignment
Does conversion volume support smart bidding?
Are shared budgets masking control levers?
Are promotions reflected in creative and landing pages?
Are landing pages aligned with intent?
Is there a measurable gap between current performance and executive expectations?
We build a centralized performance map that aligns platform signals with business reality.
Where Healthcare Attribution Typically Breaks
Attribution in healthcare almost always fails at the definition layer.
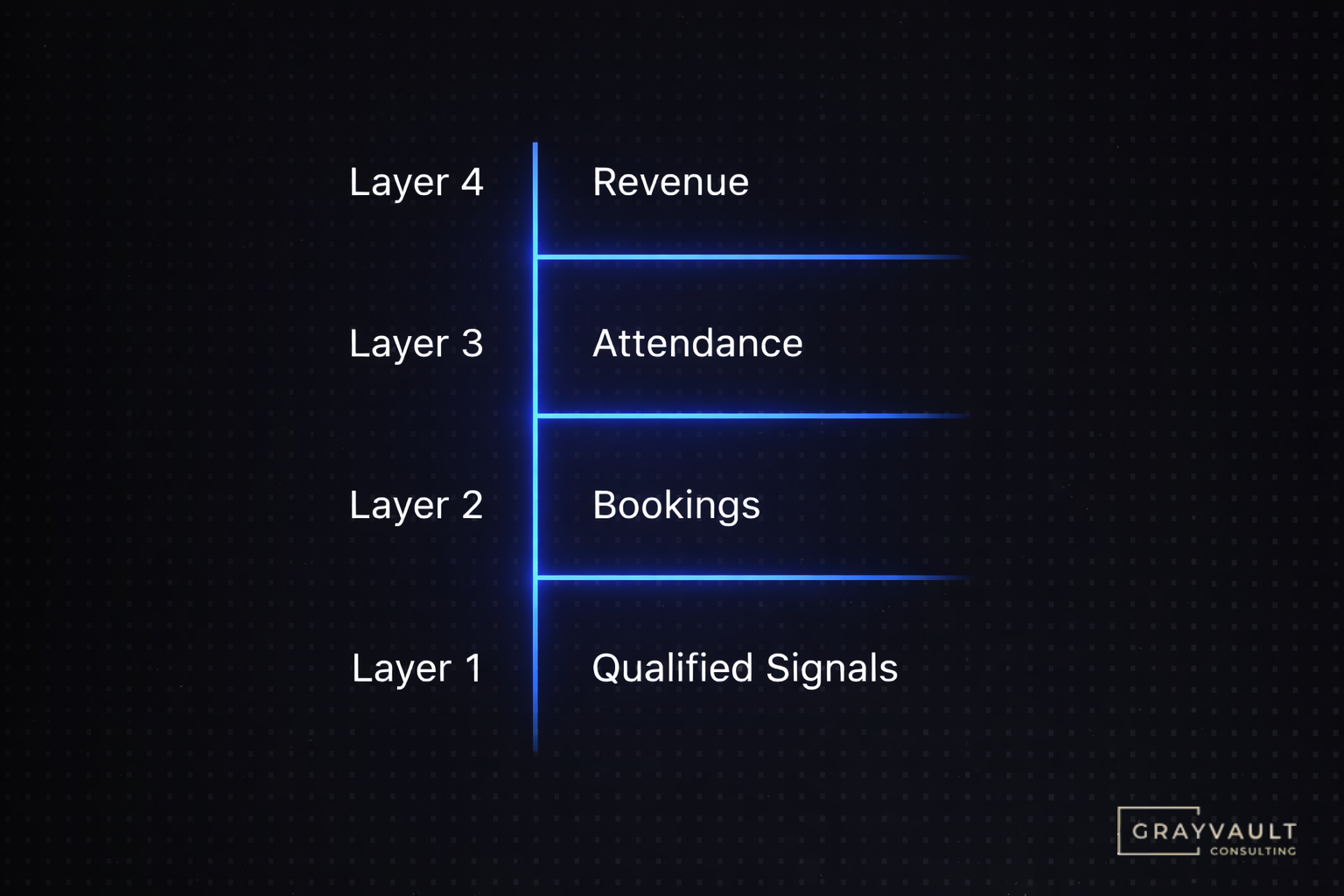
A mature paid media system typically includes four layers:
Qualified front-end signals
Calls, forms, appointment requests
Confirmed bookings
Scheduled appointments
Attendance or show rate tracking
Patients who arrive
Production-level attribution
Revenue generated
In orthodontics, these may align with case start, case start dismissed, and contract start milestones.
In other healthcare verticals, terminology differs.
The architecture principle remains identical.
Most organizations never move beyond Layer 1, often due to fear of privacy constraints or due to a lack of resources or technical knowledge.
In complex multi-location healthcare systems, performance rarely falls apart because of any one thing.
When performance deteriorates, the cause is almost always structural.
Healthcare leaders deeply understand operations, compliance, and staffing. Paid media often gets treated as a channel rather than infrastructure.
Infrastructure requires:
Defined conversion architecture
Transparent account ownership
Respect for compliance
Realistic attribution expectations
Executive patience
When those elements align, performance stabilizes.
For DSOs and multi-location healthcare brands, the real question is not:
“How do we get more leads?”
It is:
“Is our system capable of scaling responsibly?”
- Craig Graham
Founder, Grayvault Consulting
Healthcare Paid Media Glossary
DSO (Dental Support Organization)
A multi-location healthcare organization providing centralized operational and marketing support to affiliated practices.
Case Start
In orthodontics and some DSOs, a scheduled appointment that initiates a potential treatment journey. Terminology varies across healthcare.
Case Start Dismissed
A patient who attends their scheduled appointment. Often used in orthodontic reporting.
Contract Start
The point at which treatment begins and revenue is formally recognized. Sometimes referred to as treatment acceptance or production start.
Conversion Architecture
The structured hierarchy of defined conversion actions inside advertising platforms that ladder from front-end engagement to downstream revenue outcomes.
Healthcare Attribution
The process of connecting advertising interactions (clicks, calls, form submissions) to booked appointments, attended visits, and production revenue.
HIPAA-Compliant Marketing Infrastructure
Advertising and data systems designed to protect patient information, including compliant CRM integrations, privacy-safe call tracking, secure CDPs, and defined governance processes.
Scale-Ready Paid Media System
A paid media environment with stable data flow, defined governance processes, compliance safeguards, sufficient conversion volume, and executive alignment on growth timelines.
Frequently Asked Questions About Google Ads for Multi-Location Healthcare Organizations
How should Google Ads be structured for a multi-location healthcare organization? Google Ads structure should reflect business structure. If each location operates under its own domain and brand identity, separate accounts may be appropriate. If locations operate under an umbrella brand, a consolidated account with segmented campaigns by location often creates better data consolidation and bidding stability. The structure must support clean attribution, location-level visibility, and scalable governance.
What breaks attribution in healthcare Google Ads accounts? Attribution most commonly breaks at the conversion definition layer. When conversion actions do not ladder toward real business outcomes such as scheduled appointments, attended visits, or production revenue, optimization becomes disconnected from performance reality. Gaps in CRM integration, offline conversion uploads, or HIPAA-compliant data infrastructure further weaken attribution integrity.
What does “scale-ready” mean in healthcare paid media? Scale-ready means the organization has stable conversion architecture, clean data governance, compliant data handling practices, and sufficient conversion volume to support smart bidding. It also requires executive alignment around performance timelines and market opportunity. Increasing budget without these foundations often creates volatility rather than growth.
Why is HIPAA compliance important in paid media systems? Healthcare advertising often involves patient data, call tracking, CRM integrations, and conversion tracking mechanisms. Without HIPAA-compliant systems and proper data governance, organizations risk financial penalties and reputational damage. Modern healthcare paid media requires privacy-first infrastructure, not retroactive fixes.
How long does it take to stabilize a multi-location Google Ads account? Most mature accounts require at least 60 to 90 days of stable data flow to generate reliable optimization patterns. Abrupt structural changes or budget shifts can reset learning phases. Stability, structured testing, and consistent measurement are critical to sustainable performance improvement.
.svg)




.svg)
.png)

.svg)