Earlier this year I attended Women in DSO in Las Vegas, an event bringing together leaders and experts from top DSO’s.
One topic that kept coming up was leads (whether there were enough of them, whether they were high-quality enough). But in my experience, leads aren't necessarily the problem when it comes to DSOs. Neither is lead volume. What's actually dragging down DSO marketing performance is the intake process.
Where Most DSO Marketing Performance Breaks Down
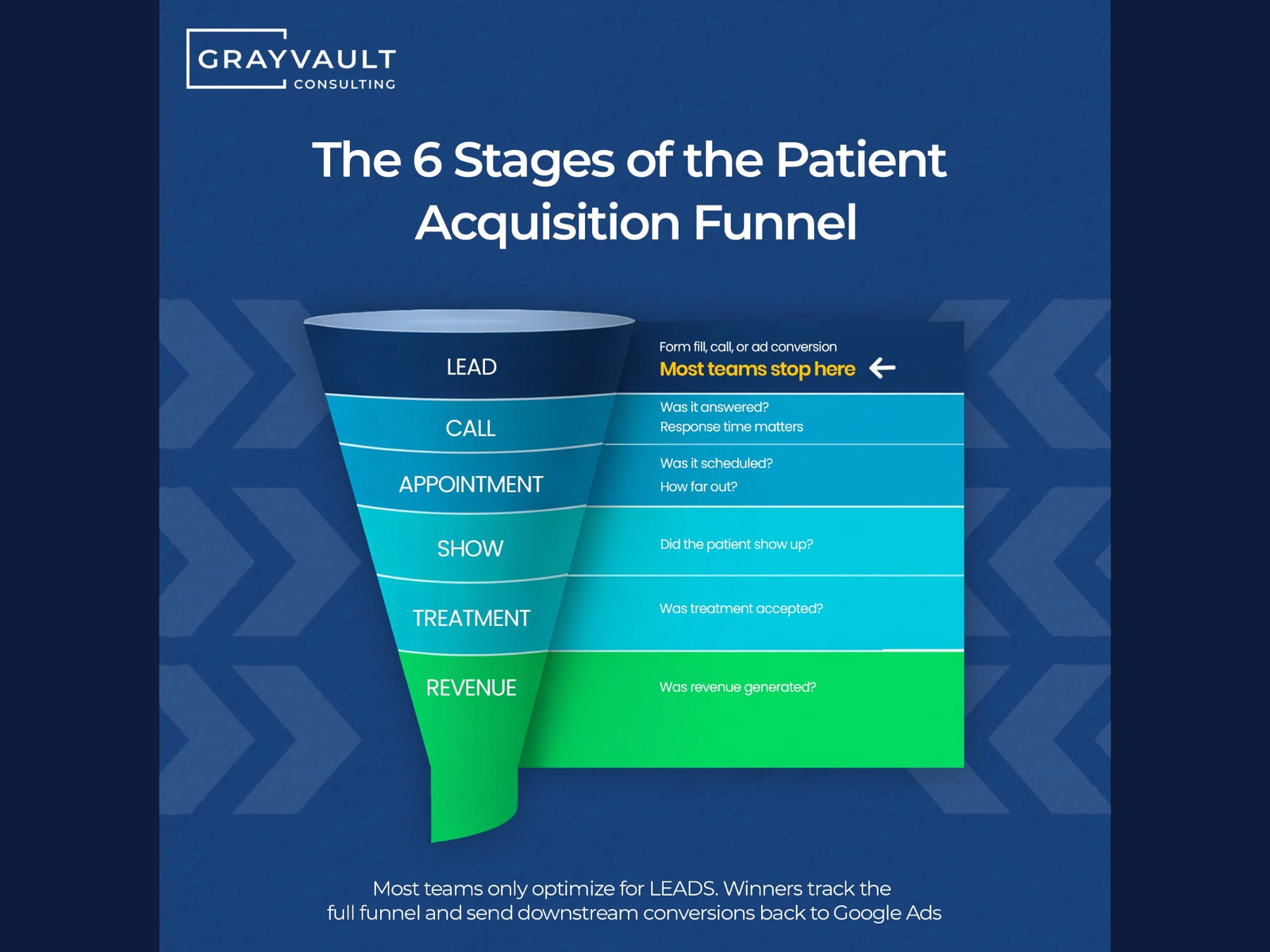
The typical DSO patient funnel has six steps:
- Lead — a form fill, phone call, or ad conversion
- Call — was it answered? How quickly? By whom?
- Appointment — was it scheduled, and how far out?
- Show — did the patient actually arrive?
- Treatment — was case acceptance completed?
- Revenue — did production hit the books?
Most teams only optimize for Step 1 and that’s where things stall. On the surface, you get a funnel that looks broken at the top. But where it’s actually broken is in the middle. And then what happens? Budget keeps going into lead generation. Leads keep coming in. And production stays flat because the system between the lead and revenue is leaking. This is one side of a bigger measurement gap, the other being why DSOs can't connect ad spend to contracted patients.
The other thing I see when I look at DSO paid media accounts, too many of them are bringing in the wrong leads. Irrelevant traffic and low-quality conversions dilute the funnel. So if you fix the quality problem at the top, everything downstream gets easier. That starts with optimizing for booked appointments rather than raw leads.
Below the lead, there are five other areas where patient acquisition breaks down:
- Unanswered calls.
Average dental practices miss somewhere around 20% of new-patient inbound calls. Phones ring during lunch, between shifts, or simply during high-volume periods and nobody picks up. A patient who called your practice and got no answer will call a competitor within minutes.
- Slow response to form fills.
The research on speed-to-lead is unambiguous: the likelihood of reaching a prospect drops dramatically with every hour that passes after they submit a form. A lead that isn’t contacted within the first few hours is, in most cases, already gone. Most DSO intake processes aren’t built around this reality.
- Poor phone scripting.
Getting the call answered is only half the problem. The person answering it needs to be able to convert an inquiry into a booked appointment. What “poor scripting” actually looks like in practice: front desk staff who lead with insurance questions before establishing any connection, who can’t clearly articulate the value of the practice, or who default to “let me check with the doctor” when a patient asks something simple. The call gets answered and the patient still doesn’t book.
- Scheduling delays.
This one is underappreciated. A patient who calls and can’t get an appointment for three or four weeks is not a converted patient. They’re a patient who will call someone else. Capacity constraints at individual locations can effectively negate all the marketing spend directed at those locations because the practice couldn’t absorb the volume.
Why Marketing Becomes the Scapegoat for Intake Failures
The reason intake failures consistently get attributed to marketing is structural, not political.
Leads are the most visible metric in any paid media system. They show up in dashboards, agency reports, platform analytics, you name it. CPL is easy to calculate, easy to benchmark, and easy to present to leadership. When leadership wants to know if DSO marketing performance is working, CPL and lead volume are the numbers that surface.
Intake failures, by contrast, happen downstream — in call logs, CRM data, and scheduling systems that often live in a completely separate part of the organization. That data doesn’t flow back into the marketing dashboard. Nor does it connect to the ad spend. So when a CMO asks why the marketing budget isn’t generating production, the honest answer is “because the phones aren’t being answered and the booking system can’t handle the volume.” Unfortunately, that answer isn’t visible in the data available to them.
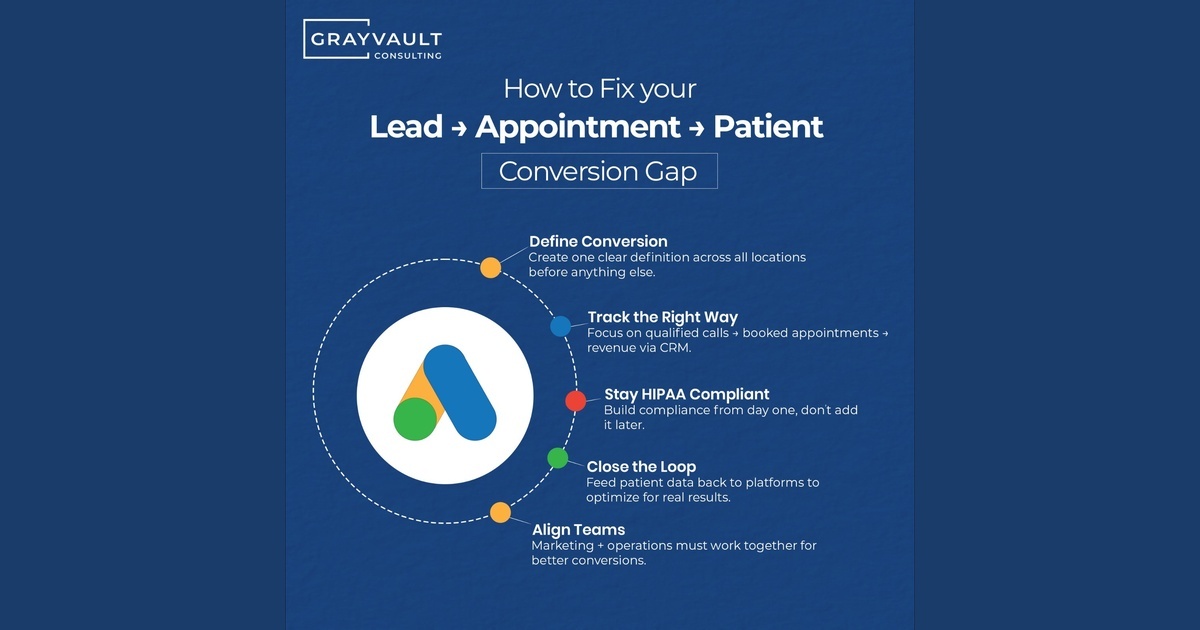
There’s also an organizational dynamic at play. Marketing and operations report to different leaders, sit in different meetings, and are measured on different KPIs. In that structure, the conversation about what happens between lead and chair doesn’t happen naturally. It has to be deliberately built through shared metrics, regular cross-department reviews, and a clear set of procedures that both teams are accountable to.
What It Looks Like When Marketing and Operations Are Finally Measuring the Same Thing
Organizations that grow efficiently don’t just optimize the top of the funnel. They optimize every stage and have the measurement infrastructure to know which stages need attention.
On the marketing side, that means conversion tracking that extends beyond the lead. Cost per booked appointment. Show rates by campaign and by location. Case acceptance rates connected back to the traffic sources that drove them. If you’re spending on paid media and you can’t answer those questions, you’re flying blindly. Getting there safely also means having the HIPAA-compliant stack to move that data without exposure.
On the operations side, it means intake accountability: call answer rates, speed-to-contact, booking conversion rates, and capacity tracking that connects to your media allocation. These metrics exist in most DSO tech stacks — they just aren’t being pulled together in a way that lets marketing and operations make decisions from the same picture.
What We Found When a Client Asked Us to Improve Their DSO Marketing Performance
A while ago, we worked with a large DSO with 500+ locations across the United States. They came to us with a straightforward brief: improve marketing performance and generate more patient appointments.
What we found when we got inside the accounts told a more complicated story:
Phones weren’t being answered consistently. When they were answered, the DSO had no reliable system for converting inquiries into booked appointments. And at a significant number of locations, the real constraint wasn’t lead quality or intake at all, but capacity.
Clinics that were already at capacity kept receiving leads. Patients were being booked three and four weeks out. At that point, they’d call a competitor who could get them in sooner. In essence, the leads weren’t converting because the practices couldn’t absorb them.
We ended up building a capacity-aware allocation model by routing budget and leads to clinics that could actually take patients on, while pulling back from locations that were overcommitted. This was more than just a media or campaign fix. This was an approach that took into account their entire operations and systems in order to ensure their success.
Three Numbers That Tell You Whether Your Problem Is Media or Intake
If you’re trying to figure out if you have a media problem or an intake problem, consider these numbers:
- If you’re spending more than $150-$300 to acquire a new dental patient and lead quality looks reasonable, start looking downstream before you adjust the media.
- If your show rate is below 60%, the problem is almost certainly not in the campaigns.
- If you’re seeing strong CPL at some locations and weak CPL at others with similar campaigns, capacity or intake consistency is almost always the differentiator.
None of this is a reason to stop investing in paid media. It’s just a reason to make sure the system that receives those leads is built to convert them before you scale the spend.
Not Sure Where Your Process is Breaking Down?
Grayvault Consulting specializes in paid media strategy and attribution architecture for DSOs and multi-location healthcare organizations. If you want to evaluate where your own funnel is breaking down, schedule a free consultation with me here.
Frequently Asked Questions
- Why is my DSO's marketing not generating more patients? In most cases, the problem isn't the marketing — it's what happens after the lead arrives. Unanswered calls, slow follow-up, poor phone scripting, and scheduling delays are the most common reasons paid media spend fails to convert into booked appointments and production revenue.
- What is a healthy cost per acquisition for a dental patient? The average CPA for a new dental patient ranges from $150–300 depending on market and location. If you're spending toward the higher end of that range and lead quality looks reasonable, the issue is likely downstream in your intake process rather than in the campaigns themselves.
- What show rate should a DSO expect from paid media leads? If your show rate is below 60%, the problem is almost certainly not in the campaigns. Show rate is primarily an intake and operations metric — driven by scheduling delays, confirmation processes, and how well the practice communicates with patients between booking and appointment.
- Why do marketing and operations teams at DSOs measure different things? Marketing and operations typically report to different leaders, sit in different meetings, and are measured on different KPIs. This structural gap means the data that explains why leads aren't converting — call answer rates, booking conversion, capacity constraints — rarely surfaces in a way that connects back to marketing spend.
- How do you fix a dental practice intake problem? Start by auditing every stage of your patient acquisition funnel, not just lead volume and CPL. Track call answer rates, speed-to-contact, booking conversion rates, show rates, and capacity by location. Once you can see where patients are being lost, you can build systems to stop losing them there before scaling spend.
.svg)



.png)
.svg)


.svg)